Where Would I Find Cubs Beer and Wine
Don't miss out on the latest nutrition and supplement research
Enter your email and we'll keep you on top of the latest nutrition research, supplement myths, and more.
Study under review: Grape or grain but never the twain? A randomized controlled multiarm matched-triplet crossover trial of beer and wine
You are reading a free Examine article. Become a Member to get full access to all our articles and stay on top of the latest research.
Introduction
Alcohol-induced hangovers (medically known as veisalgia) are the feeling of general misery people get on the day after excessive drinking. You may be familiar with some of the symptoms [1]: headache, dry mouth, nausea, gastrointestinal distress, and dizziness. Typically, the hangover begins within several hours after drinking stops, when a person's blood alcohol concentration (BAC) begins to drop, and with symptoms usually peaking at around the time BAC is back to zero.
The exact reason why alcohol causes a hangover is not well-understood, but it seems that immune, hormone, and dehydration-related factors [2] are involved. More specifically, scientists have been looking at the following putative mechanisms [3]: (i) alcohol's direct effects on electrolyte balance, gastric irritation, low blood sugar (hypoglycemia), sleep disturbances, cytokine and prostaglandin production, dehydration, and vasodilation, and (ii) alcohol's indirect effects on oxidative status through alcohol metabolites, such as acetaldehyde, and through congeners (substances that are present in alcoholic drinks), such as amines, amides, acetones, polyphenols, methanol, and histamine.
Despite the fact that hangovers seem to have important socio-economic costs [4] in terms of absenteeism from work, lower productivity or work performance, work-related accidents, interpersonal conflicts, and academic underperformance, little research exists on how hangovers may be managed or prevented. A 2017 systematic review [5] of the few available human trials concluded that a handful of herbal products may potentially help in the treatment and/or prevention of hangovers. However, none of them were effective in relieving all hangover symptoms. The main results are shown in Figure 1.

With little relevant available research, most people rely on anecdotal evidence and on old sayings for finding ways to prevent or treat hangovers. One such saying, which exists in several languages, relates to the order of beer and wine consumption. In English, the saying goes "Beer before wine and you'll feel fine; wine before beer and you'll feel queer." Similarly, the Germans say, "Wein auf Bier, das rat' ich Dir—Bier auf Wein, das lass' sein," and the French say "Bière sur vin est venin, vin sur bière est belle manière." Since there are currently no scientific data to support or refute this statement, the study under review set out to do just that, by comparing the effect of the order of beer and wine consumption on next-day hangover severity.
Alcohol-induced hangover is the feeling of general misery people get on the day after excessive drinking, a problem that's associated with important socio-economic costs like work absenteeism. Yet, little research exists on how hangovers may be managed or prevented. To test whether the type and order of drinks influences hangover development, the study under review compared the effects of the order of beer and wine consumption on next day hangover severity.
Who and what was studied?
This was an non-blinded, randomized, crossover trial involving 90 participants (45 men and 45 women) aged 19-40 years old, with an average BMI of 22, average alcohol consumption rate of once weekly, and average hangover frequency of once monthly.
Due to the nature of the experiment, participants with a history of drug or alcohol abuse, liver dysfunction, and a variety of diseases were excluded. Participants with an aversion to beer or wine, a history of complete alcohol abstinence or intolerance, and people of East Asian descent and corresponding genetic polymorphisms that reduce their ability to metabolize alcohol were likewise excluded.
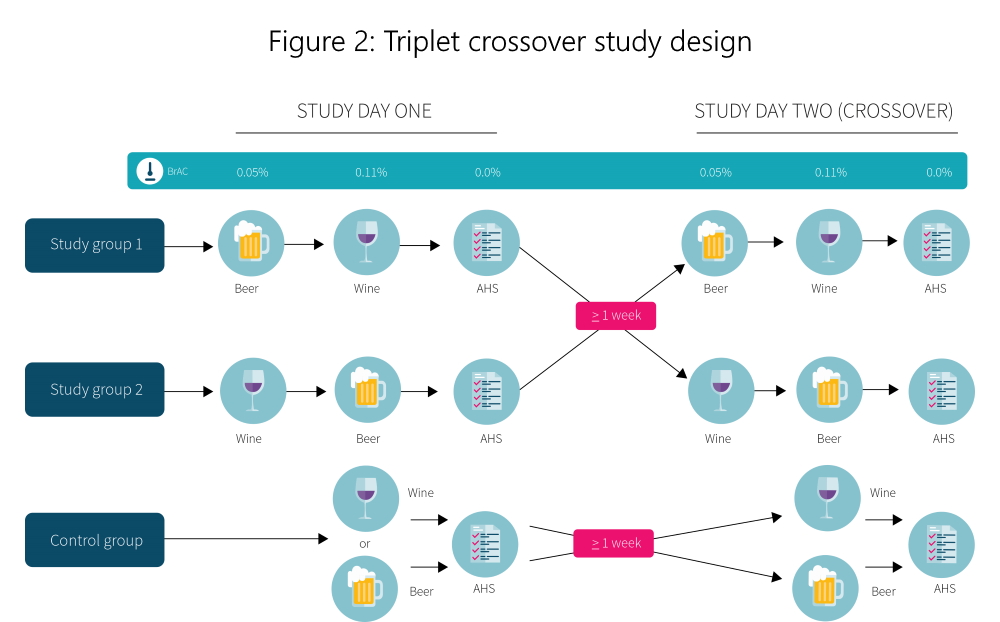
The participants were matched into triplets based on age, gender, weight, height, BMI, reported alcohol consumption rate, and hangover frequency, and then randomly assigned to one of three groups: study group 1 (drink beer followed by wine, n=31), study group 2 (drink wine followed by beer, n=31), or a control group (drink either only beer or only wine, n=28). The triplet and crossover design helped increase the power of the study relative to other possibilities (like a parallel design, which would have required more people). The study was designed to have an 80% power to detect a 14% difference in the Acute Hangover Scale (AHS), which required 36 participants per group.
The primary outcome was the reported hangover severity on the day following each intervention, which was measured using the Acute Hangover Scale [6] (AHS). This scale uses an eight-item compound score (including thirst, fatigue, headache, dizziness, nausea, stomach ache, tachycardia, and loss of appetite), with each item rated by participants on a scale of 0 to 7. Secondary outcomes included factors associated with hangover intensity (e.g., demographics, laboratory parameters, etc.). The study was not pre-registered.
The study design is depicted in Figure 2. On the first intervention day, participants in study group 1 consumed beer up to a breath alcohol concentration (BrAC) of at least 0.05% and then drank wine to a BrAC of 0.11%, while participants from study group 2 consumed wine first and then beer to comparable BrAC levels. The control group participants consumed only beer or wine. Upon completion of the intervention, all participants received an individualized amount of water (six milliliters per kilogram of bodyweight) to be consumed before going to sleep at the study site. On the next day, after the BrAC had returned to zero, hangover severity was assessed using the AHS. On the second intervention day, which took place after a one-week washout, each group was crossed over to the opposite regimen, and the experiment was repeated.
All participants were asked to refrain from consuming alcohol for one week before each intervention, and to consume food and water as per usual on intervention days. Before each intervention, all participants received a standardized meal tailored to their gender- and age-specific estimated energy requirements.
In this open-label, randomized, crossover trial, 90 healthy men and women drank beer followed by wine or wine followed by beer on two separate occasions. On the next day, after breath alcohol concentration (BrAC) had returned to zero, hangover severity was assessed using the Acute Hangover Scale [6] (AHS). The primary outcomes assessed were differences between the interventions for hangover severity, while secondary outcomes included factors associated with hangover intensity (e.g., demographics, laboratory parameters, etc.).
What were the findings?
There were no significant differences between any of the groups for hangover severity, even when the researchers adjusted the AHS relative to the peak BrAC reached for each participant. It's important to note, however, that a large number of participants dropped out before the follow-up, which meant the study ended up being underpowered to detect changes in the primary outcome.
For secondary outcomes, a statistically significant difference was found for AHS ratings between women and men, with women reporting increased hangover severity. However, the significance disappeared after adjusting AHS ratings for the variation in peak BrAC. Moreover, further analyses revealed that perceived drunkenness and vomiting were the strongest predictors of hangover intensity, while factors such as age, sex, drinking habits, and peak BrAC reached did not help reliably predict hangover intensity.
It's also worth mentioning that participants drank, on average, around 1.3 liters of beer and 0.65 liters of wine during each intervention, which amounts to around eight standard drinks, in order to reach the target BrAC level.
No significant differences were found for hangover severity differences between interventions, which was the primary outcome. For secondary outcomes, it was found that perceived drunkenness and vomiting were the strongest predictors of hangover intensity, while factors such as age, sex, drinking habits, and peak BrAC reached did not help predict hangover intensity.
What does the study really tell us?
The results of the study suggest that the order of beer and wine consumption is unlikely to have an effect on next-day hangover severity, and do not confirm the popular saying of "Beer before wine and you'll feel fine; wine before beer and you'll feel queer." The results also suggest that perceived drunkenness and vomiting after alcohol consumption are useful predictors of next-day hangover severity. Despite the study's relatively strong design, several methodological limitations are worth discussing.
In order to assess hangover severity, the researchers used an eight-item rating scale called the Acute Hangover Scale [6]. This is one of the three commonly used hangover scales, the other two being the Alcohol Hangover Severity Scale [7] and the Hangover Symptoms Scale [8]. Each scale lists different hangover symptoms, with fatigue, thirst, and nausea being the only three symptoms, out of a total of 22, that are listed by all three scales. Although the overall hangover severity scores of the three scales correspond [7] quite well, it would be interesting to see if different results would be obtained had another scale, or a combination of the three scales, been used.
With the AHS, participants rate eight items on a scale of 0 to 7, and then the ratings of individual items are added together to get a total score out of 56. A score of zero represents the absence of any hangover symptoms, while a score of 56 corresponds to the worst hangover imaginable. In the study under review, the hangover severity of the study groups was between 16 and 17, which represents a relatively mild hangover severity. This ties in well with the fact that the peak breath alcohol concentration reached was 0.12-0.13%, which isn't low, but which could be higher. It would be illuminating to determine whether a higher breath alcohol concentration and, consequently, higher next-day overall hangover severity, would help tease out any potential small differences between interventions.
Another limitation worth mentioning pertains to the sample size. Although a power analysis was conducted by the researchers to estimate the number of participants needed per group to detect a 14% difference between groups (i.e., a two to three point difference on the AHS scale), a large number of participants dropped out before the follow-up due to exams and holidays, which resulted in a smaller-than-needed sample size. More specifically, while the power analysis showed that a minimum of 36 participants were needed per group, only 31 were left in each study group, and 28 were left in the control group. This means that, although the study rules out the existence of very large differences between groups, the sample size was likely too small for a statistically significant difference between groups to be detected even for a between-group difference larger than 14%.
The lack of blinding can also be considered as a limitation. As human behaviour is influenced by what we know or believe, it is anticipated that research results can be affected by the participants' expectations. Blinding [9] participants to a treatment is used to eliminate this bias. In the study under review, participants were not blinded as, according to a pre-trial performed by the researchers, it was not feasible to do so. It is, of course, logical to assume that if a bias had existed, it would probably be in favor of supporting the notion that having beer after wine would lead to more severe hangover symptoms, as this is what the popular saying claims. Since the study did not find support for this claim, the lack of blinding isn't much of a problem.
Finally, it's important to consider the generalizability of the results. Firstly, the study used lager beer and white wine, so it's possible that different results could have been obtained if different brands or types of beer and wine had been used. Different results could have also been found if hard liquor (e.g. tequila, rum, and brandy) or mixed drinks had been evaluated, in part due to the potential effects congeners [10] can have on hangover severity. Moreover, the participants were young and middle-aged healthy men and women of non-Eastern Asian origin, who had an average alcohol consumption rate of once weekly, and average hangover frequency of once monthly. As such, the findings of the study cannot be extrapolated to other populations, including people of Eastern Asian origin, the elderly, or people who consume alcohol or experience hangovers much less or more frequently than the participants in this study. Future studies could address some of the above limitations by using larger sample sizes, including hard liquor, and assess the effects of a broader range of blood alcohol concentrations.
The study under review suggests that, in young and middle-aged men and women of non-Eastern Asian origin, the order of wine and beer consumption has no effect on next-day hangover severity, and that perceived drunkenness and vomiting after alcohol consumption are useful predictors of how hungover people are likely to feel on the next day. However, considering the study's limitations, its limited generalizability, as well as the fact that this was the first study of its kind, the case may not be closed.
The big picture
This was the first study to have examined the order of wine and beer consumption on hangover severity, which means that there are no other studies to directly compare the results to. Moreover, although there are currently no proposed physiological mechanisms for why the order of drinking beer and wine should affect hangover severity that can be examined, there's still some literature investigating the causes of hangover that may help put these findings into some perspective.
As mentioned earlier, suggested causes of hangover symptoms include the direct and indirect effects of alcohol consumption on the body.
Most hangover symptoms appear [3] to be due to direct effects of alcohol, such as alcohol-induced electrolyte imbalances, hormonal alterations, gastric irritation, hypoglycemia, sleep alterations, vasodilatation, and cytokine production. For example, headaches [11] may be explained by alcohol-induced increases in serotonin, histamine, and prostaglandin levels, while memory impairments [12] may be explained by an increase in cytokine production. The increase in pro-inflammatory cytokine production, which is thought to be due to an alcohol-induced increase in thromboxane B2 [13] levels, may also explain symptoms such as nausea, diarrhea, and tiredness.
With the above research in mind, it makes sense to assume that higher breath alcohol concentration levels should correlate with increased severity of hangover symptoms. However, the study under review reported that a correlation between BrAC and hangover intensity was not observed. While the researchers rightly point out that the range of peak alcohol levels studied were too narrow for a link to be detected and that a link probably exists, the results from other studies on the matter are conflicting, with some research [14] finding no significant correlation between peak blood alcohol concentration and hangover severity, and with other research [15] reporting a significant relationship between hangover severity and the administered dose of alcohol. Individual physiology may also play a role here, with a 2016 study [16] reporting that a significant association between alcohol levels and hangover severity was found in participants who experienced a hangover, while this association was not detected in participants who claimed to be hangover-free, despite reaching the same peak blood alcohol concentration levels.
The indirect effects of alcohol consumption on hangovers are thought to mainly be a result of acetaldehyde, an alcohol metabolite, and congeners, substances that color and flavor drinks.
After alcohol consumption, the alcohol is metabolized [17] and converted into acetaldehyde, which is then further metabolized to acetate. Though acetaldehyde is present in the blood for a short period of time, it is highly reactive and can cause tissue damage due to its toxic effects [18], which may lead to hangover-like symptoms such as nausea, sweating, rapid pulse, and headache. While acetaldehyde blood concentration during the most severe period of a hangover is low, it may be the case that it acts during the drinking process and promotes a delayed [19] effect that leads to the experienced hangover symptoms once the analgesic effects of alcohol are gone.
Congeners are substances that naturally occur in alcoholic beverages or are added during the production process, and include amines, amides, acetones, polyphenols, methanol, and histamine. Congeners are thought to contribute to hangover severity through their toxic effects. In line with this, research [20] suggests that alcoholic drinks with higher congener contents, such as red wine, whiskey, and tequila, increase hangover severity more than drinks with lower congener contents, such as white wine, gin, beer, and vodka. For example, in an older study [21], 91 young and middle-aged participants received vodka (low congener content) or bourbon (high congener content). At lower blood alcohol concentration levels, there was no detectable difference between vodka and bourbon with regard to their capacity for inducing hangover. However, at blood alcohol concentration levels of 0.10-0.15%, a severe hangover was reported by 33% of participants who drank bourbon, and only by 3% of participants who drank vodka, while mild to moderate hangover was reported by more people after vodka (61%) than after bourbon (44%). This suggests that, while vodka was enough to produce a mild to moderate hangover, bourbon's predominant effects were in increasing the incidence of a severe hangover. The levels of congeners in various drinks are shown in Figure 3.
Figure 3: Congener content of various drinks

Reference: Verster JC. Alcohol Alcohol. 2008 Mar. [1]
In the study under review, lager beer and white wine were used, both of which contain relatively low levels of congeners [1]. However, at the time that the age-old saying about the order of wine and beer consumption first appeared, it is likely that different types of wine and beer were used, which possibly contained different levels of congeners, and which could have played a role in hangover severity with different drink consumption orders.
Excluding the study under review, there are no studies examining the effects of beer and wine consumption order on hangover severity. If the totality of the available research is taken into consideration, including the study under review, there don't seem to be biologically plausible arguments or any scientific data which suggest that drinking different alcoholic drinks in any particular order should affect hangover severity. Instead, what primarily seems to affect hangover severity is the total volume of alcohol consumed, as well as the content of congeners present in the drink.
Frequently asked questions
Q. How long do hangovers usually last?
There is surprisingly little research examining alcohol-induced hangover duration. One 2018 survey study [22] in male and female students aged 18-30 years old found that, for the majority of drinkers, the duration of the alcohol hangover ranged from 14 to 23 hours, with an average duration of around 18 hours after stopping drinking. The study also reported a significant correlation between hangover severity and duration.
Q. Why were people of Eastern Asian origin excluded from the study?
People of Eastern Asian descent have higher rates of a mutation in the aldehyde dehydrogenase (ALDH2) gene [23], which can lead to more severe hangover symptoms. More specifically, the ALDH2 gene plays a role in metabolizing acetaldehyde into acetate. The common form of ALDH2 is ALDH2*1, while the variant form is ALDH*2 (i.e., the mutation mentioned above). This variant is believed to decrease conversion rates of acetaldehyde to acetate during alcohol metabolism, leading to an excess build-up of acetaldehyde. As we've discussed in the previous section, acetaldehyde is highly reactive and can cause tissue damage due to its toxic effects [18], which is how it's thought to contribute toward hangovers. Since people of Eastern Asian descent have a higher prevalence of the ALDH2*1 variant, they tend to experience more severe hangover symptoms, which would affect the study results.
Q. What's the evidence for some other anti-hangover remedies?
A number of hangover preventatives and remedies have been investigated, and a few have shown promise in helping prevent or treat some symptoms. Hangover cures with some scientific support for their efficacy include tolfenamic acid [24], Siberian ginseng [25], Korean pear juice [26], red ginseng [27], dandelion juice [28], and prickly pear extract [29], some of which were covered by the systematic review mentioned in the introduction.There are also several commercial preparation formulas [30]. According to the limited available evidence, these products may improve some hangover symptoms, mainly those related to the central nervous system, gastrointestinal distress, and dehydration.
The purported mechanisms through which the above remedies may act involve the facilitation of alcohol metabolism, reduction of oxidative stress, and controlling of inflammation. However, these mechanisms have not been well investigated. Moreover, most of the studies on the cures mentioned above are of poor methodological quality and have never been replicated.
Overall, reliable scientific evidence supporting the use of any purported hangover remedy is lacking. It seems that the best way to prevent a hangover is to simply drink in moderation and, preferably, on a full stomach. In case you've already drank too much, staying hydrated and getting enough sleep should be your priorities.
What should I know?
Alcohol-induced hangover is the feeling of general misery people get on the day after excessive drinking. Although hangovers may have important socio-economic costs, research on how they may be managed or prevented is lacking. Instead, people rely on anecdotal information and on old sayings such as "Beer before wine and you'll feel fine; wine before beer and you'll feel queer." To test whether this saying is true, the study under review compared the effects of the order of beer and wine consumption on next day hangover severity.
The results suggest that, in young and middle-aged men and women of non-Eastern Asian descent, the order of drinking wine and beer is unlikely to have an effect on next-day hangover severity, although the study was underpowered to detect small differences. The study also found that perceived drunkenness and vomiting after alcohol consumption can predict how hungover people are likely to feel on the next day. A generally good idea to prevent hangovers is to simply drink in moderation and avoid alcoholic drinks with a very high congener content.
You are reading a free Examine article. Become a Member to get full access to all our articles and stay on top of the latest research.
See other articles with similar topics: Beer, Wine, Alcohol, Congeners.
See other articles in Issue #53 (March 2019) of Study Deep Dives.
References
- ^ a b c Verster JC. The alcohol hangover--a puzzling phenomenon. Alcohol Alcohol. (2008)
- ^ Penning R, et al. The pathology of alcohol hangover. Curr Drug Abuse Rev. (2010)
- ^ a b Prat G, Adan A, Sánchez-Turet M. Alcohol hangover: a critical review of explanatory factors. Hum Psychopharmacol. (2009)
- ^ Verster JC, et al. The alcohol hangover research group consensus statement on best practice in alcohol hangover research. Curr Drug Abuse Rev. (2010)
- ^ Jayawardena R, et al. Interventions for treatment and/or prevention of alcohol hangover: Systematic review. Hum Psychopharmacol. (2017)
- ^ a b c Rohsenow DJ, et al. The Acute Hangover Scale: A new measure of immediate hangover symptoms. Addict Behav. (2007)
- ^ a b Penning R, et al. Measurement of alcohol hangover severity: development of the Alcohol Hangover Severity Scale (AHSS). Psychopharmacology (Berl). (2013)
- ^ Slutske WS, Piasecki TM, Hunt-Carter EE. Development and initial validation of the Hangover Symptoms Scale: prevalence and correlates of Hangover Symptoms in college students. Alcohol Clin Exp Res. (2003)
- ^ Day SJ, Altman DG. Statistics notes: blinding in clinical trials and other studies. BMJ. (2000)
- ^ Rohsenow DJ, Howland J. The role of beverage congeners in hangover and other residual effects of alcohol intoxication: a review. Curr Drug Abuse Rev. (2010)
- ^ Pattichis K, et al. 5-Hydroxytryptamine release from platelets by different red wines: implications for migraine. Eur J Pharmacol. (1995)
- ^ Reichenberg A, et al. Cytokine-associated emotional and cognitive disturbances in humans. Arch Gen Psychiatry. (2001)
- ^ Kangasaho M, et al. Effects of ethanol intoxication and hangover on plasma levels of thromboxane B2 and 6-keto-prostaglandin F1 alpha and on thromboxane B2 formation by platelets in man. Thromb Haemost. (1982)
- ^ Ylikahri RH, et al. Metabolic studies on the pathogenesis of hangover. Eur J Clin Invest. (1974)
- ^ Kruisselbrink LD, et al. Physical and psychomotor functioning of females the morning after consuming low to moderate quantities of beer. J Stud Alcohol. (2006)
- ^ Van de Loo A, et al. Urine ethanol concentration and alcohol hangover severity. Psychopharmacology (Berl). (2017)
- ^ Zakhari S. Overview: how is alcohol metabolized by the body?. Alcohol Res Health. (2006)
- ^ a b Eriksson CJ. The role of acetaldehyde in the actions of alcohol (update 2000). Alcohol Clin Exp Res. (2001)
- ^ Chauhan BL, Kulkarni RD. Alcohol hangover and Liv.52. Eur J Clin Pharmacol. (1991)
- ^ Rohsenow DJ, et al. Intoxication with bourbon versus vodka: effects on hangover, sleep, and next-day neurocognitive performance in young adults. Alcohol Clin Exp Res. (2010)
- ^ Chapman LF. Experimental induction of hangover. Q J Stud Alcohol. (1970)
- ^ The Duration of the Alcohol Hangover.
- ^ Eng MY, Luczak SE, Wall TL. ALDH2, ADH1B, and ADH1C genotypes in Asians: a literature review. Alcohol Res Health. (2007)
- ^ Kaivola S, et al. Hangover headache and prostaglandins: prophylactic treatment with tolfenamic acid. Cephalalgia. (1983)
- ^ Bang JS, et al. Clinical effect of a polysaccharide-rich extract of Acanthopanax senticosus on alcohol hangover. Pharmazie. (2015)
- ^ Lee HS, et al. Effect of Korean pear (Pyruspyrifolia cv. Shingo) juice on hangover severity following alcohol consumption. Food Chem Toxicol. (2013)
- ^ Lee MH, et al. Red ginseng relieves the effects of alcohol consumption and hangover symptoms in healthy men: a randomized crossover study. Food Funct. (2014)
- ^ Effect of Dandelion Juice Supplementation on Alcohol-Induced Oxidative Stress and Hangover in Healthy Male College Students.
- ^ Wiese J, et al. Effect of Opuntia ficus indica on symptoms of the alcohol hangover. Arch Intern Med. (2004)
- ^ Takahashi M, et al. Clinical effectiveness of KSS formula, a traditional folk remedy for alcohol hangover symptoms. J Nat Med. (2010)
Where Would I Find Cubs Beer and Wine
Source: https://examine.com/members/deep-dives/article/beer-before-wine-or-wine-before-beer/
0 Response to "Where Would I Find Cubs Beer and Wine"
Post a Comment